My Sick Liver
Esophageal Varices
Esophageal varices are extremely dilated veins in the lower esophagus (throat). They most often are a consequence of portal hypertension, commonly due to cirrhosis. Patients with esophageal varices have a strong tendency to develop bleeding, which, could be life-threatening if left untreated.



Esophageal Varices Development
The majority of blood from the esophagus is drained via the esophageal veins. These veins have no part in the development of esophageal varices. The remaining blood from the esophagus is drained through a series of veins into the portal vein. These superficial veins, normally only about 1 mm in diameter, become enlarged (up to 1–2 cm in diameter) causing portal hypertension. Blood flow begins to bypass the normal paths the lower esophagus, abdominal wall, stomach and rectum. The small blood vessels in these areas swell and expand, becoming more thin-walled, and appear as permanently dilated veins (varicosities). In addition, these vessels are poorly supported by other structures, as they are not designed for high pressures.
Varices can also form in other areas of the body, including the stomach (gastric varices), duodenum (duodenal varices), and rectum (rectal varices).
Esophageal Varices Treatment
In emergency situations, care is directed at stopping blood loss, maintaining plasma volume, correcting clotting problems induced by cirrhosis, and appropriate use of antibiotics as infections can easily occur. Restoring blood volume should be done promptly and with caution so as to avoid increasing portal pressure leading to more bleeding. Restoring the lost blood can also worsen ascites and increase portal pressure.
Therapeutic endoscopy is considered the mainstay of urgent treatment. Two main therapeutic approaches exist: variceal banding (also called ligation) and sclerotherapy.
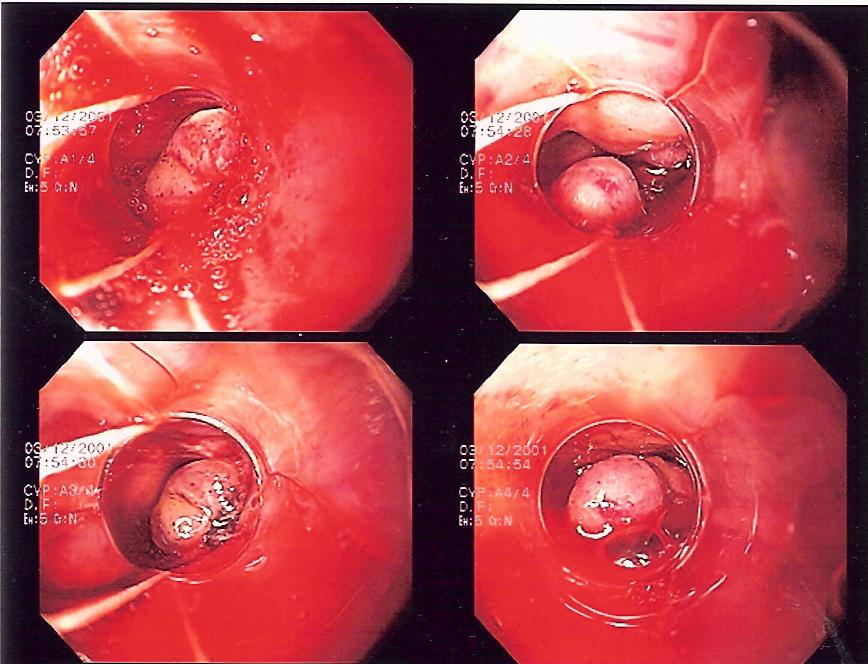
During endoscopic variceal banding, a doctor uses an endoscope to place an elastic ring that looks like a rubber band around an enlarged vein. Banding the vein in this manner will cut off blood flow through the vein. It may be difficult to use this procedure while someone is actively bleeding, because the device used to place the bands obscures the doctor's vision. Variceal banding can be as effective as sclerotherapy in treating episodes of bleeding and it has fewer complications.
Variceal banding is often done several times to control the varices and prevent bleeding. For example, banding might be repeated every 2 to 4 weeks for 3 to 4 sessions.
During endoscopic sclerotherapy, a chemical called a sclerosant is injected directly into an enlarged vein or into the wall of the esophagus next to the enlarged veins. The substance causes inflammation of the inside lining of the vein, which over time causes the vein to close off and scar. When the vein is closed off, blood cannot flow through it. Endoscopic sclerotherapy may be effective for stopping immediate (acute) bleeding caused by esophageal varices.
Sclerotherapy is still done in emergencies, but it is not as popular as it was in the past. More than before, doctors are using variceal banding to treat and prevent esophageal variceal bleeding. Even if sclerotherapy is done at first, variceal banding is usually done later to prevent future bleeding. Both procedures work. But variceal banding has less chance of complication than sclerotherapy.
The majority of blood from the esophagus is drained via the esophageal veins. These veins have no part in the development of esophageal varices. The remaining blood from the esophagus is drained through a series of veins into the portal vein. These superficial veins, normally only about 1 mm in diameter, become enlarged (up to 1–2 cm in diameter) causing portal hypertension. Blood flow begins to bypass the normal paths the lower esophagus, abdominal wall, stomach and rectum. The small blood vessels in these areas swell and expand, becoming more thin-walled, and appear as permanently dilated veins (varicosities). In addition, these vessels are poorly supported by other structures, as they are not designed for high pressures.
Varices can also form in other areas of the body, including the stomach (gastric varices), duodenum (duodenal varices), and rectum (rectal varices).
Esophageal Varices Treatment
In emergency situations, care is directed at stopping blood loss, maintaining plasma volume, correcting clotting problems induced by cirrhosis, and appropriate use of antibiotics as infections can easily occur. Restoring blood volume should be done promptly and with caution so as to avoid increasing portal pressure leading to more bleeding. Restoring the lost blood can also worsen ascites and increase portal pressure.
Therapeutic endoscopy is considered the mainstay of urgent treatment. Two main therapeutic approaches exist: variceal banding (also called ligation) and sclerotherapy.
During endoscopic variceal banding, a doctor uses an endoscope to place an elastic ring that looks like a rubber band around an enlarged vein. Banding the vein in this manner will cut off blood flow through the vein. It may be difficult to use this procedure while someone is actively bleeding, because the device used to place the bands obscures the doctor's vision. Variceal banding can be as effective as sclerotherapy in treating episodes of bleeding and it has fewer complications.
Variceal banding is often done several times to control the varices and prevent bleeding. For example, banding might be repeated every 2 to 4 weeks for 3 to 4 sessions.
During endoscopic sclerotherapy, a chemical called a sclerosant is injected directly into an enlarged vein or into the wall of the esophagus next to the enlarged veins. The substance causes inflammation of the inside lining of the vein, which over time causes the vein to close off and scar. When the vein is closed off, blood cannot flow through it. Endoscopic sclerotherapy may be effective for stopping immediate (acute) bleeding caused by esophageal varices.
Sclerotherapy is still done in emergencies, but it is not as popular as it was in the past. More than before, doctors are using variceal banding to treat and prevent esophageal variceal bleeding. Even if sclerotherapy is done at first, variceal banding is usually done later to prevent future bleeding. Both procedures work. But variceal banding has less chance of complication than sclerotherapy.
